By Slobodan Despot. Antipresse 230, 26.4.2020. Permalink
The pandemic of this spring 2020 is not just a health issue. It may even be more socio-political than medical. The virus is coupled with a “system error” in all developed countries that has led to a panicky management of the crisis defying common sense. In this interview without masks or gloves, Dr Jean-Pierre Spinosa summarizes the health problem and outlines a possible therapeutic approach.

Is it necessary to write a list? The disorganization of health services, the shortage of masks and disinfectant in the best-equipped countries, the war being waged on those seeking effective treatments for this disease without a hypothetical vaccine, the omission of the strengthening of individual immunity in practically all official communication on the subject, and finally the blatant inconsistency and stupidity of certain authorities mean that the epidemic can no longer be separated from a particularly dilapidated “civilizational” context.
The misadventure suffered by Swiss health anthropologist Jean-Dominique Michel is one of the best illustrations of this decay. When he was publishing an article now become viral, “Playing down the current epidemic” (1), JDM tested positive and began therapy under the guidance of his treating physician. The sequence of events, which he detailed in his blog (2), is staggering. In a nutshell: the patient’s condition worsening, his doctor prescribed Dr Raoult’s treatment – which proved to be unavailable, as it was reserved for hospitals (where generally patients arrive in a condition too advanced for this therapy). Michel had to organize, via his wife, “an illegal transaction, at the edge of a parking lot” to obtain Plaquenil (hydroxychloroquine) and start his treatment at home. The result was that he was back on his feet on the sixth day.
Yes, this is 2020 in Switzerland, one of the most medicalized countries in the world!
What would have happened to Jean-Dominique Michel without this drug transaction at the edge of a parking lot? He must have asked himself that a thousand times before writing words as these:
“Yes, you read it right: the governments of Switzerland and France (and unfortunately other countries as well) have left hundreds of people to die, depriving them of a simple, well-known and inexpensive treatment, which must be given at the beginning of a SARS-CoV-2 infection.
What have our authorities been doing for more than a fortnight now that the effectiveness of this treatment has been confirmed? Well, they have found nothing better than reserving stocks of hydroxychloroquine for the hospital, making it impossible for general practitioners to prescribe it and keeping it for people for whom it is already too late, even though the relevant indication is to prescribe the treatment before the complications occur, precisely to prevent them.
Are we simply measuring not merely the absurdity, but also the monstrosity of the thing?!”
Absurdity and monstrosity! At the end of his ordeal, this balanced mind published a poignant and frightening questioning of the reasons for the hydroxychloroquine blockage. Speaking of obstructions, we have since learned that the basic blood test for antibodies, as part of the detection of the virus, is not covered by Swiss health insurance! Individuals are charged for a basic gesture of collective health protection! This is simply unimaginable.
It is difficult, in the face of such facts, not to believe in conspiracies. To stay within the boundaries of reason, and not limit myself to my own speculations, I decided to give the floor to a doctor who is passionate about research, cancerology and biochemistry.
Since the beginning of this crisis, I’d been in conversation with Dr Jean-Pierre Spinosa. He is the author, with Catherine Riva, of a landmark book, even though it was stifled by the media: An Injection too many? (Xenia, 2010.) The rigorous analysis that the two authors provided at the time of the crisis of how the industry had “sold” a vaccine with questionable and contested efficacy to governments may help to understand some key aspects of the current crisis.
I asked him the questions that everyone is asking, from our retired parents to doctors in shock. On the basis of his experience, Dr Spinosa sketched out hypotheses guided by observation and common sense that at the very least deserve to be examined.
What are we dealing with?
JPS:
Let’s be honest: I don’t know. The information we receive is incomplete and contradictory, and I can only repeat what I have heard. I can only see the effects of what is happening to us: the measures we are taking, the social and economic repercussions. I do not see the dead. I’m not an emergency doctor.We have a peak year for respiratory diseases, as were 2015 and 2017. According to figures from the FSO (Swiss Federal Statistical Office), the number of deaths per week remains in a zone of comparable amplitude (3). What differs is the unprecedented scale of these protective measures and the subsequent panic.

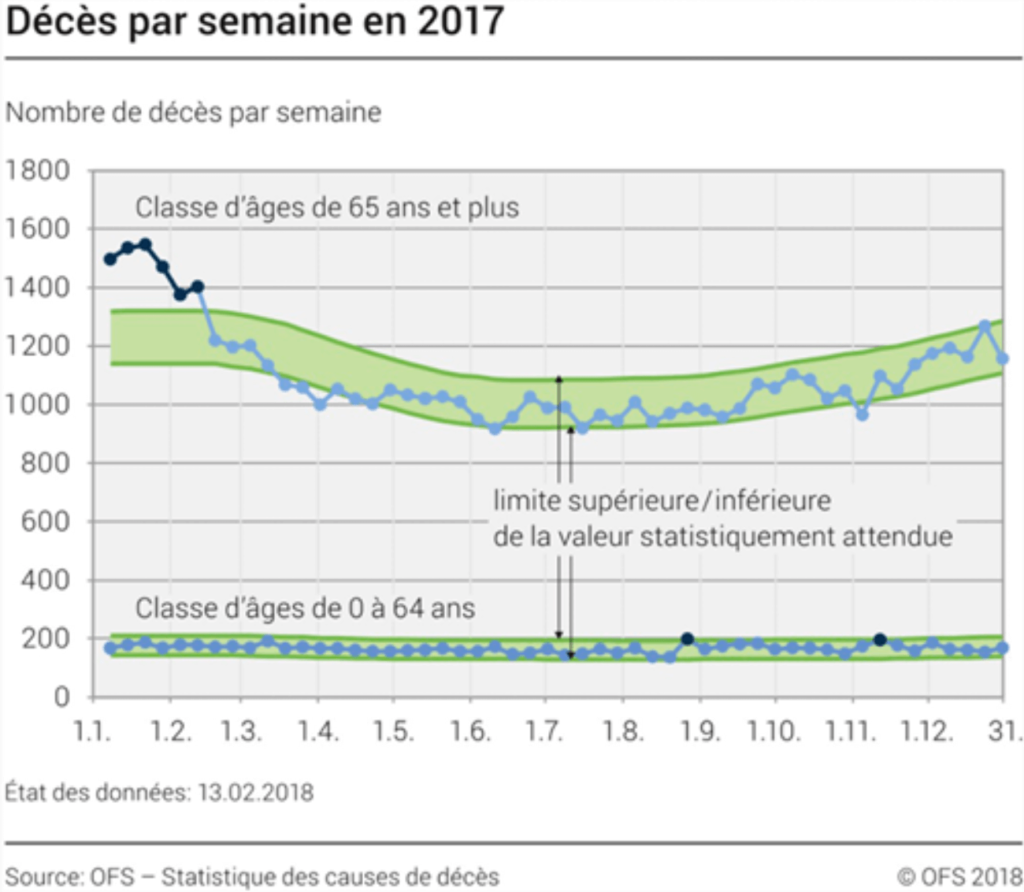
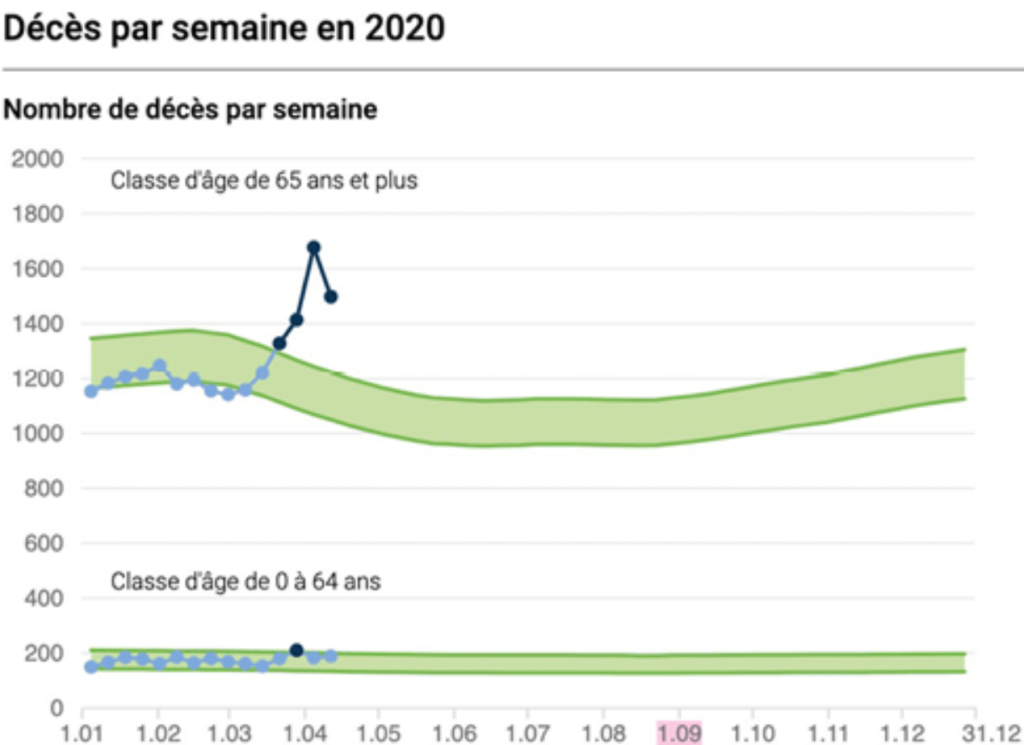
Mortality statistics 2015-2017-2020 in Switzerland, according to the FSO. Apart from a time lag of about one month, the mortality in spring 2020 remains in line with previous years.
Long before this interview, Dr Spinosa, who closely follows events in his home country, Italy, had drawn my attention to the media dramatization of what was happening there. The truly critical situation in Bergamo was used as a paradigm of the seriousness of the scourge – so much so that the CBS channel, in a crude and unsanctioned “fake news”, has used images from Bergamo to illustrate the crisis… in the United States. In this confusion, no one wondered why the other regions of Italy were much less affected. The focus on the virus invoked as an incantation masked all the other parameters of the Bergamo tragedy: the fact that the air in the highly industrialized Po Valley was the most polluted in Europe, that the health system was seriously deficient… but also that it boasted of having massively vaccinated the elderly in several waves in previous years. It was as if somebody wanted to put Italy and the whole of Europe in the “all-out panic” mode denounced by the statistician W. M. Briggs.
JPS:
Officially, the SARS-CoV-2 virus (let’s be precise: that’s its name, COVID-19 being the name of the disease) is believed to trigger pneumonia with a greater lethality than previous respiratory illnesses. In the panic, an unfortunate and misplaced connection was made with the so-called Spanish flu of 1918.
When Hippocrates’s medicine gave way to spreadsheet medicine…
How do you explain these mistakes in the treatment of a disease that may ultimately prove to be quite manageable?
JPS:
The WHO (an association of political and not medical bodies, it should be remembered) declared from the outset that COVID-19 was a respiratory disease of viral origin. It therefore explicitly discouraged doctors from treating their patients with antibiotics… because we have been taught that only bacterial pneumonia can be treated with antibiotics. If this description is correct, there is no way to attack this virus. In practical terms, this leaves the doctors only the possibility of treating the symptoms, supporting the vital functions. However, it has been claimed that anti-inflammatory drugs have a harmful role because they “facilitate the attacks” of the virus against cells: the choice of symptomatic treatments has even been limited. Basically, people were left alone with their disease. They consulted too late, when they had reached a stage that was difficult to catch up on. Others, on the other hand, did not consult, even in serious situations. This is how Swiss cardiologists noticed a sharp drop in emergency consultations for heart attacks and other serious problems. In the absence of antivirals, by advising against antibiotics and without heparin (anticoagulant), a slide to intensive care was created. The emergency doctors had to face an absurd and desperate situation, with admirable self-sacrifice, but without asking any questions.In this case, more than one doctor would have had the reflex to prescribe antibiotics – but this would have been a provocative act under WHO guidelines. Thus, in northern Italy, according to some professionals, the strict application of stupid instructions has led to inept treatment and thus to a large number of deaths.
An anomaly called Raoult
And yet the only treatment that seems to be working so far is antibiotics…
JPS:
Yes. There was a grain of sand in the machine called Didier Raoult. Raoult is an old and titled anarchist (which did not protect him from an attempt to throw him out by the Council of the Order of Physicians). He is one of the most respected virologists in the world. He could afford to blow the whistle on the WHO and his own government. Although I do not agree with his position in favour of the Gardasil vaccine, which I have studied well, it must be acknowledged that his approach, in this case, was both humane and Hippocratic. Treatment first, with the means at hand!In order to do so, he had first to overcome the sacrosanct rule of the EBM (Evidence Based Medicine) i.e. the need to prove the effectiveness of a double-blind treatment. Obviously too tedious a procedure in this situation of absolute urgency, but one that the authorities insist on with fanatical rigour. Raoult reasoned as a war physician: “In the absence of the possibility of proof, is it more legitimate to treat on the basis of biological plausibility, or to abstain because my treatment is not validated?” If there were a validated EBM protocol, of course he would have applied it, but since there is no validated EBM protocol, he can’t just sit and do nothing. He thinks that the combination azithromycin + hydroxychloroquine has a possibility to succeed. He thinks like a doctor, not an administrator. He practises field medicine, as most practitioners do every day. In these situations, you don’t think about what the Excel spreadsheet is going to look like.
There’s something surprisingly mechanical and even antimedical about this protocol approach to medicine…
JPS:
At the very least. In the last twenty years, the medical art has changed a lot. In the past, the doctor had to choose the most suitable treatment for the patient with the patient’s consent. Today, recommendations and guidelines have to be applied. Doctors are bombarded with recommendations from the administrative authorities or the WHO, recommendations that we do not know who wrote them. As soon as they stray from these ruts, they assume responsibility that will be theirs if there is a problem with legal complaints. In real life, however, there are always glitches, even when we do our best. Medicine is locked into a mandatory pathway that few have the courage to break out of, especially among young people who cannot afford to jeopardize their future careers.We must now be able to justify all the reasons for a treatment or intervention. It is virtually impossible to go against the current, knowing that any deviation, even if it is proven to work, carries a degree of risk. The doctor-patient relationship has evolved to a triangle in which the statistician, flanked by the administrator and the lawyer, is becoming increasingly important.
This being said, the sacrosanct rule of the EBM often has variable geometry. Where are the EBMs that motivate the wearing of masks and gloves, the social distancing, the rules of confinement? When one country sets the distance at 2 metres and another at 1 metre, are we dealing with two different viruses, the first more contagious than the second? Or are we simply acting in total improvisation and ignorance?
The Lessons of HPV
The structure of the problem is therefore beginning to emerge: comprehensive health management is like a pyramid of national sub-pyramids. Decisions taken at the top, which must be accepted as unquestionable truths, cascade down the ladder to your family doctor. It was by studying how states were convinced, from top to bottom, of the need for Gardasil, the “vaccine against cervical cancer” caused by the papillomavirus (HPV), that Jean-Pierre Spinosa understood the calamitous mechanics of failure in the face of the coronavirus of 2020. A mechanism of bureaucratization on a governmental and planetary scale coupled with dispossession. The mastery of the medical art is no longer in the hands of doctors.
JPS:
The Gardasil story can help us understand the political and economic aspects of the current crisis. It is one of the most expensive vaccines ever produced and is endorsed by many states, especially the richer ones. Yet the EBM studies available on it have not proven its effectiveness in reducing dysplasia (precancer). The question of its dangerousness also arises, although the studies are discordant on this subject.Virologically, the papillomavirus conundrum presents an interesting analogy for understanding the current disease. Why does HPV not cause cancer in all the women it affects, but only in some? The same question arises in 2020 with SARS-CoV-2, which primarily targets older men with serious chronic comorbidities (pathologies) such as diabetes, hypertension and obesity.
In the case of the HPV, the gearing seems more precise. The presence of HPV is associated with the development of cervical cancer depending on the microbiota (type of microbial flora) that exists in the patient’s vagina. In other words, the presence of certain bacteria causes an imbalance that favours the appearance of precancers by a mechanism that is still poorly understood. Especially in the last ten years or so, increasingly important publications have shown an association between the presence of certain (anaerobic) bacteria, the persistence of HPV and the risk of developing cervical cancer. A 2018 publication in the prestigious journal Nature confirmed it and on March 4th I came across a publication by some Madhivanan which indicates that a bacterium by the name of Prevotella is associated with the persistence of HPV and possibly the development of precancer.
Based on my research on HPV, I asked myself the same question about the serious complications of coronavirus. Is there also an “intermediary” or “accomplice”, possibly bacterial, that the virus could “infect”, and that would be involved? In the literature, I have come across cases where there is a recurrent association of serious illness (or death) between coronavirus infection and anaerobic bacteria, i.e. bacteria that develop only in the absence of oxygen. A brilliant researcher, former UC Davis Sandeep Chakraborty, a specialist in computational biology, has uncovered some very interesting information about this subgroup. He determined genetic traces of one of these bacteria, Prevotella, in samples from people with severe COVID-19. A second scientist, who calls himself Biomoon without revealing his real name, confirmed this. This tends to reinforce the hypothesis that I share with other researchers around the world that the coronavirus may not be the cause of the serious manifestations of the disease, but a trigger/amplifier.
Observing anaerobic bacteria puts new pieces in place that leave you puzzled. For example, Prevotella, although present in everyone’s airways, can trigger very serious pneumonia. Studies show that it is even capable of attacking haemoglobin. However, one of the striking manifestations of COVID-19 described by medical intensivists is a dramatic lack of oxygen. An American emergency doctor confronted with this phenomenon immediately alerted his colleagues with a very explicit video: patients suddenly start gasping for air as if they were at an altitude of 8,000 m. Prevotella makes the haemoglobin “inactive”, as in a rarefied atmosphere. It can also cause microthromboses. And it is involved in the famous “cytokine storm” described in the seriously ill.
This raises the question as to why autopsies were not performed immediately, as early as 2019, on the first patients who died of this disease. Microembolisms would probably have been detected, and this complication might have led us earlier to the trail of bacterial superinfection by Prevotella. And it is not excluded that these autopsies could have shown the presence of the coronavirus long before the theoretical start date of the epidemic.
But if this lead were to be confirmed, the treatment of COVID-19 would have to change dramatically…
JPS :
Indeed. The treatment by support therapy and ventilation recommended by the WHO would then prove to be wrong. Some even go so far as to say that it might worsen the patient’s condition. On the contrary, it would be a question of 1) strengthening individual immunity (big debate…); 2) administering an antibiotic targeting anaerobes; 3) administering an anticoagulant; 4) providing a possible antiviral when it is available… All this while waiting for the arrival of a vaccine which will have proved its effectiveness in randomized studies. This completely changes the paradigm.At the same time, we are nearing to the treatments set up by Professor Raoult (minus heparin), as well as Doctor Sabine Paliard Franco (3) in France and Dr Vladimir Zelenko (5) in New York, and which are the only ones to date to give results.
Who’s the murderer, after all?
For many weeks, Dr Spinosa had been tracking a publication that allowed him, like HPV and the vaginal microbiota, to identify this bacterium named Prevotella. Bernard Dugué had also spotted the possible assassin. Reactions in the medical and media mainstream were not long in coming: “Fake news!” Even before EBM had made its first attempt on this channel, it was blocked because it was contrary to WHO recommendations. It is as if an attempt was being made to rule out, as they appear, all alternatives to universal and compulsory vaccination – with a vaccine that does not yet exist!
JPS:
It is essential to recognize that it is not the virus that kills the patient, but the hyperactive immune system that is “unbalanced”.At least three pathological mechanisms lead to multi-organ failure and death in COVID-19:
1) An exaggerated inflammatory reaction called “cytokine storm” with damage to the lungs, kidneys and heart.
2) Exaggerated coagulability (increased clotting). The hypothesis is that the deregulated immune system damages the vessel wall and activates blood clotting, causing the formation of micro and macro blood clots (thromboses) in the lungs and other organs, hence early treatment with anticoagulants (e.g. Heparin).
3) A low level of oxygen in the blood as a result of the above.
In light of all this, it can be deduced that the high morbidity and mortality attributed to COVID-19 are due, among other things, to the widespread and inappropriate reluctance to make prompt use of anti-inflammatory and anticoagulant treatments, including corticosteroid therapy at the beginning of a patient’s hospitalization, and an appropriate antibiotic therapy aimed at anaerobes.
Prevotella is currently a hypothesis. But it is the hypothesis that today accounts for most of the elements described and known. It should therefore not be underestimated, but more studies should be carried out quickly to confirm or refute it.
Will reality be stronger than ideology, bureaucratic interference and conflicts of interest? We will see in the coming months, but the battle has begun. Our entire future may depend on it. We can emerge from this ordeal through health and medical means by identifying effective therapies and rebuilding health systems that are clearly devastated. But we can also get out of it technologically by introducing widespread population surveillance “for security’s sake”. After COVID-19, we’ll have VIDCO-21, DIVOC-23… there’s no reason why the scarecrow trail should stop.
What would the technological outcome so fervently favoured by the ruling elites bring us? Apart from the civic regression that would make us de facto renounce human rights and freedom of thought and accept a lasting infantilization, it would be a rather saddening insight, as expressed at the end of our interview by Dr Spinosa:
JPS:
What do we see in 2020? That in this particular case, with the exception of the tremendous progress made in intensive care and the discovery of antibacterials, we have not made much progress in preventing the spread of epidemics since the plagues of past centuries. Containment, isolation, coercion, quarantine (forty days already prescribed by Hippocrates!) Why is it that with all the billions invested in research and technology we find ourselves so ignorant and helpless in the face of a single virus? This raises serious questions about the failure of technological medicine and the decline of civilization that some scientists are already predicting. What education, what schooling, what social relations will we offer to young people in this world of fear and regression?
Notes
- “Covid-19, game over”, March 18, 2020.
- “Covid: how many needless deaths (and how I cured myself with hydroxychloroquine)?!” , 5.4.2020.
- Curve 2015, Curve 2017, Curve 2020.
- http://covid.ueuo.com
- https://www.liberation.fr/checknews/2020/04/03/plus-de-600-patients-new-yorkais-ont-ils-ete-gueris-du-covid-19-en-mars-grace-a-l-hydroxychloroquine_1784084_
©2020 Antipresse.net. Original article: «Coronavirus, l’erreur système» (Antipresse.net n° 230, 26.4.2020). About | Subscribe.